Canalicular adenoma is a type of growth that occurs in human salivary glands. It is a benign growth which occurs in the epithelial cells, and is typically arranged in columns of cells that form interconnecting cords. Canalicular adenoma is a very rare benign neoplasm; it constitutes about 1% of all salivary gland tumors and about 4% of all benign salivary gland tumors.[1][2]
Presentation
editCanalicular adenoma is most common in patients age 70 to 80, with females affected about four times as often as males. Most growths present in the upper lip; some also occur in the a few present in palate or buccal (cheek) tissue as a slowly enlarging mass.[3] The growths will often arise in multiple places at the same time or develop multiple nodes, despite not being clinically invasive or malignant.[1][4]
Diagnosis
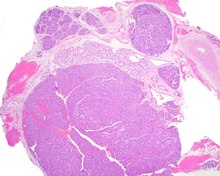
editCanalicular adenoma growths are usually small at the time they are noticed, with an average size of about 1.6 cm.[1] Their histologic appearance is very distinct, with a channel-like pattern between cords and ribbons; the pattern has been described as resembling a "string of pearls."


The growths often contain are often small bight squamous balls, or morules. They also typically contain a well-developed supporting tissue - a fibrous stroma - which is rich in hyaluronic acid and chondroitin sulphate.[1] In a few cases, the growths may contain small calcium deposits or microliths. Although it is seldom necessary, a pathologist can confirm the existence of canalicular adenoma through immunohistochemistry studies, with the cells reacting with pancytokeratin, S100 protein and SOX10, with a delicate GFAP reaction around the periphery.[5][1][6][7] Although it is a benign tumor, a positive diagnosis of canalicular adenoma may be necessary to exclude the existence of other medical conditions such as a basal cell adenoma, pleomorphic adenoma, adenoid cystic carcinoma, and polymorphous adenocarcinoma.
Treatment
editMost instances of canalicular adenoma are treated with conservative surgery.[1]
References
edit- ^ a b c d e f Thompson LD, Bauer JL, Chiosea S, McHugh JB, Seethala RR, Miettinen M, Müller S (Jun 2015). "Canalicular adenoma: a clinicopathologic and immunohistochemical analysis of 67 cases with a review of the literature". Head Neck Pathol. 9 (2): 181–195. doi:10.1007/s12105-014-0560-6. PMC 4424207. PMID 25141970.
- ^ Nelson JF, Jacoway JR (Jun 1973). "Monomorphic adenoma (canalicular type). Report of 29 cases". Cancer. 31 (6): 1511–1513. doi:10.1002/1097-0142(197306)31:6<1511::aid-cncr2820310630>3.0.co;2-o. PMID 4709966. S2CID 71093824.
- ^ Suarez P, Hammond HL, Luna MA, Stimson PG (Aug 1998). "Palatal canalicular adenoma: report of 12 cases and review of the literature". Ann Diagn Pathol. 2 (4): 224–228. doi:10.1016/s1092-9134(98)80011-7. PMID 9845742.
- ^ Penner CR, Thompson LD (Mar 2005). "Canalicular adenoma". Ear Nose Throat J. 84 (3): 132. doi:10.1177/014556130508400306. PMID 15871577.
- ^ Ferreiro JA (Dec 1994). "Immunohistochemical analysis of salivary gland canalicular adenoma". Oral Surg Oral Med Oral Pathol. 78 (6): 761–765. doi:10.1016/0030-4220(94)90093-0. PMID 7534898.
- ^ Huebner TA, Almubarak H, Drachenberg CB, Papadimitriou JC (Apr 2014). "Canalicular adenoma--search for the cell of origin: ultrastructural and immunohistochemical analysis of 7 cases and review of the literature". Ultrastruct Pathol. 38 (2): 74–82. doi:10.3109/01913123.2013.833564. PMID 24144157. S2CID 40082155.
- ^ Curran AE, Allen CM, Beck FM, Damm DD, Murrah VA (Sep 2007). "Distinctive pattern of glial fibrillary acidic protein immunoreactivity useful in distinguishing fragmented pleomorphic adenoma, canalicular adenoma and polymorphous low grade adenocarcinoma of minor salivary glands". Head Neck Pathol. 1 (1): 27–32. doi:10.1007/s12105-007-0003-8. PMC 2807497. PMID 20614277.